From patient advocacy to clinical research, Arizona leaders are redefining Long COVID and bringing the National Institute of Health’s RECOVER study to communities across the state.

By Anisia Corona, MPH, Tanisha Prasad, and Rohan Melwani
Arizona is quietly becoming a proving ground for one of the most complex challenges in modern medicine: Long COVID. At the center of that effort are two very different leaders, patient advocate Mike Zissis of Gilbert and clinical operations expert Dr. Dallin Tavoian in Tucson. The two are helping shape how the National Institute of Health (NIH)’s national RECOVER study shows up in the state’s communities, from downtown Phoenix, to rural highways in an RV built for research.
Rethinking What Long COVID Really Is
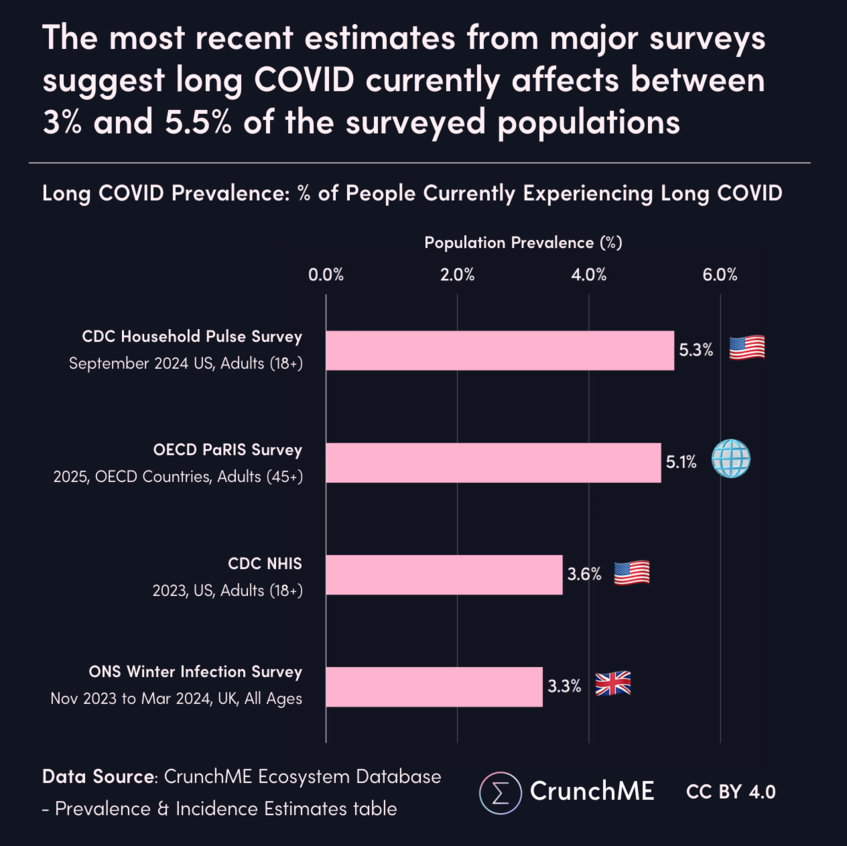
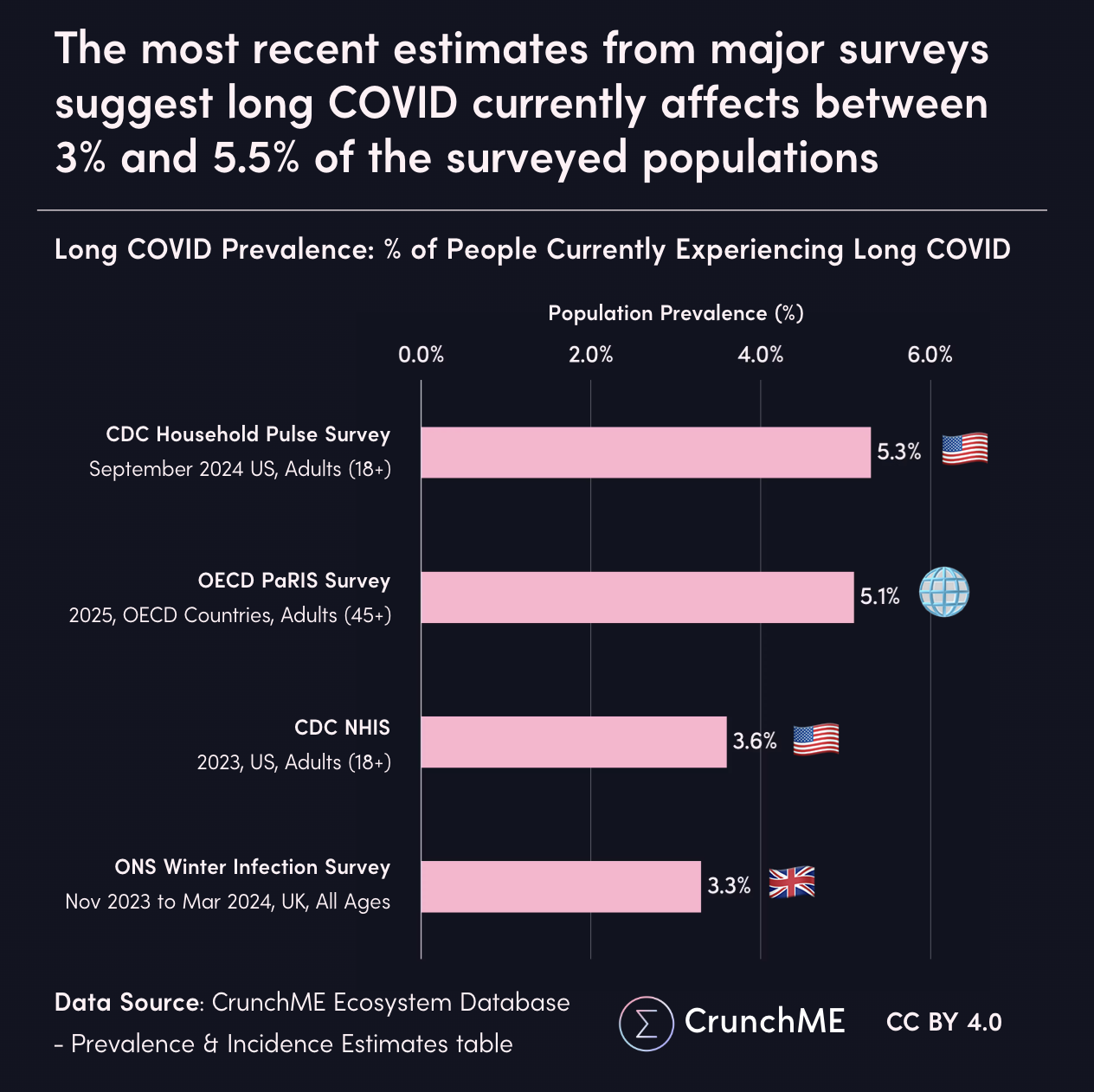
In 2020, Long COVID was often framed as a lingering lung problem: an extended tail of respiratory damage after acute infection. Six years later, evidence from RECOVER and related studies shows a more complicated reality. Long COVID now appears to be a multi-system, tissue-based disease shaped by overlapping mechanisms in 7.2% of people who get infected1.
These upstream processes can manifest downstream as tissue damage, chronic low-level hypoxia, dysautonomia, shifts in the gut–brain axis, and neurocognitive issues that show up as “brain fog,” memory lapses, difficulty multitasking, or any of the 200+ symptoms that manifest differently in everyone. A rising prevalence with each infection, increasing chances of Long COVID2, that should be a concern for any business and civic leader. For clinicians, one of the most striking lessons is that blood tests alone often fail to capture this complexity. That’s why RECOVER has invested heavily in advanced imaging and tissue-based sampling, partnering with Mayo Clinic to create one of the world’s largest repositories of organ and imaging data related to Long COVID. Because many immune processes unfold inside tissues rather than in circulating blood, these deeper samples may hold the key to explaining why two patients with similar lab panels can have very different symptom paths over time.
A recent analysis of the RECOVER-Adult cohort highlights those divergent paths. Instead of a single “Long COVID course,” researchers identified multiple trajectories: some participants improved gradually, others carried a persistent high symptom burden, and a substantial subset followed fluctuating patterns that remained severe or relapsed after reinfection3. Among participants who met research criteria for Long COVID at three months, the majority had persistent or intermittently high symptom levels over the following year. For employers and community leaders, this underscores a simple but consequential point: there is no typical Long COVID patient, and planning for the next decade means planning for variability, both in recovery time and in the support people need to stay in the workforce.
When Patients Become Co-Designers

When Long COVID cut into his daily life, Mike Zissis did something many patients never get the chance to do: he stepped directly into the engine room of national research. He enrolled in the RECOVER observational study through the University of Arizona’s Phoenix site, making the roughly 20-mile drive from Gilbert to a hospital near McDowell Road and Seventh Street, a round trip that eats about a total of two hours out of his day.
For Cissis, the drive is manageable, but he’s quick to point out that the same is not true for everyone. Many Arizonans with Long COVID symptoms face transportation barriers, limited mobility, or work and caregiving responsibilities that make regular in-person visits difficult. Every time he arrives on site, he finds a team he describes as “helpful, thorough, and compassionate,” even as staffing turnover remains an ongoing reality in a stressed healthcare workforce and limited NIH funding.
What began as participation has evolved into leadership. Zissis serves as a co-chair on the National Community Engagement Group for RECOVER and as a voting member on the Observational Cohort Steering Committee, roles that give him direct input into how protocols, priorities, and patient-facing processes are shaped. He’s also looking ahead to RECOVER’s next phase, RECOVER-TLC (short for “Treating Long COVID”), where trials will focus more heavily on testing potential treatments. His long-term goal: help build the evidence base needed to secure diagnostic codes and coverage for Long COVID therapies, so patients aren’t left fighting both their symptoms and their insurers, or facing out of pocket costs.
RECOVER has also broken new ground in how patients are embedded in the science itself. For the first time in a major NIH effort of this scale, people living with Long COVID sit not just on advisory panels, but inside nearly every layer of decision-making: they co-develop protocols, review and co-author manuscripts for publication, serve on steering and oversight committees, and help shape how findings are communicated back to the community. This deep integration has made the research more grounded in reality, pushed investigators to measure what actually matters in daily life, and built a level of transparency and trust that is rare in federally funded trials. By treating patients as partners rather than subjects, the RECOVER program has set an exemplary standard for how future complex-disease research should be designed and governed.
Cissis is clear-eyed about both the promise and the gaps. One of his biggest critiques is that research often stays locked inside academic circles instead of reaching the people it’s meant to help. “One of the biggest flaws in research is that studies are only seen by the research team,” he notes. This leaves a gap for innovation: the data has been generated, but now it must be translated into accessible care, public awareness, and real-world decisions that impact patients.
Three Sites, One Statewide Mission
If Zissis represents the voice of the participant, Dr. Dallin Tavoian, PhD represents the architecture behind the scenes. Based in Tucson, Tavoian serves as the clinical operations manager or “hub manager” for Arizona’s three RECOVER observational sites: Banner – University Medical Center Phoenix, a partner hospital site in Tucson, and the University of Arizona location.
On paper, three sites sounds modest for a state this large. In practice, it is a complex logistical operation across hundreds of miles of desert, urban neighborhoods, retirement communities, and border towns. Phoenix alone draws participants from across the metro, but Tavoian’s team also sees patients traveling from as far as Flagstaff, about a two-and-a-half-hour drive. With Arizona’s sparse geography, sprawling highways, and uneven transit options, simply getting people in the door is a challenge.
Tavoian’s answer has been to build systems. He oversees a team of roughly 18 to 20 staff across the three locations, including clinical research coordinators, some of whom have Long COVID themselves, who bring a deeply patient-centered mindset to the work. Early on, the team invested heavily in internal logistics: standardized workflows, tracking systems, and documentation that keep a complicated national protocol running smoothly at the local level.
Climate, Culture, and Who Shows Up
Arizona’s role in RECOVER isn’t just geographic; it’s demographic. Because the state sits so close to the Mexican border, the Arizona sites have a higher proportion of Hispanic participants than many other regions. That representation matters when national teams analyze Long COVID’s impact across different populations and risk profiles. For business and civic leaders focused on equity, workforce health, and regional competitiveness, it also highlights how the state of Arizona can shape more inclusive data at a national level.
The climate cuts both ways. In the summer, 110-degree days make travel and public transit particularly brutal, especially for participants with lung or cardiovascular issues. Those conditions amplify every friction point in the system, from parking and timing to the physical toll of commuting to a clinic. In the winter, however, the mild weather becomes a quiet advantage over snowbound states, allowing year-round recruitment and more consistent follow-up visits.
A Mobile Lab on Arizona’s Back Roads
To reach patients beyond the main hubs, Tavoian’s team is preparing a mobile health unit, a research-ready RV that can process blood and bring parts of the RECOVER protocol directly to rural communities. The unit is part of the CEAL (Community Engagement Alliance) program led by principal investigator Dr. Sairam Parthasarathy and is designed to extend the study’s reach into areas where a two-hour drive each way is simply not an option.
For Arizona Ascent’s readers, the mobile unit is more than a human-interest detail. It’s an example of how healthcare innovation is starting to mirror trends in other sectors: nimble, distributed infrastructure; services delivered closer to where people actually live; and partnerships that blur traditional boundaries between academic medicine, community organizations, and logistics. Imagine a research-grade RV pulling into a town that rarely sees specialists, turning a church parking lot or community center into a temporary front door to national science.
As Long COVID clinics and trials become a permanent part of the post-pandemic landscape, these mobile and hybrid models could influence how other services, from diagnostics to behavioral health, deploy across Arizona.
Data, Voice, and The Rise of AI tools
Even with deep imaging and tissue data, one gap keeps surfacing in both the science and the lived experience of Long COVID: nuance. Standard electronic health records excel at logging lab values and billing codes, but rarely capture how symptoms alter the rhythm of everyday life, whether someone can tolerate a 30-minute commute, manage childcare after work, or deliver on a sales job when brain fog hits midweek.
My Arizona-based digital health company, DxTx, is beginning to address that blind spot with a conversational AI tool that lets Long COVID patients describe their experiences in their own words from their beds or couches. These systems can turn narrative accounts into structured qualitative data, layering them onto existing clinical measures and helping surface patterns that would otherwise remain scattered across individual anecdotes.
At the same time, DxTx is curating databases that connect vetted Long COVID therapies, from rehabilitation approaches to emerging medications, to the clinical publications that support them. For busy community physicians who may only see a handful of Long COVID patients in a typical month, this kind of just-in-time, evidence-linked resource can be the difference in between telling someone “there is nothing we can do” and offering a pathway grounded in the latest science. We must bridge the data collected in research to the real world and in the hands of doctors and innovators who are making things happen.
Together, RECOVER and these emerging tools represent a new kind of health innovation ecosystem: national infrastructure and deep biology on one side, and local, AI-enabled storytelling and treatment navigation on the other. Arizona is already in the middle of that convergence; the question is how far the state is willing to lean in.
Shaping the Future of Care

On the operations side, Tavoian advocates for creating a national operations group made up of hub managers from across the country. While RECOVER already has technical committees and data groups, he argues that there is no substitute for connecting the people who handle the “boots-on-the-ground” logistics at each site. Sharing templates, playbooks, and troubleshooting lessons across hubs could accelerate everything from enrollment to retention, mirroring the way Arizona’s business community has used peer networks and accelerators to compress learning curves for founders.
Layered on top of this is a wave of new tools, from conversational AI that can capture nuanced patient stories by voice, to curated databases that tie Long COVID treatments to peer-reviewed publications. For a state leaning into its identity as a rising tech and health hub, these projects signal how Arizona can help transform patient experience into decision-grade data.
A Call to Arizona’s Leaders
Long COVID is an ongoing test for how future pandemics will play out in Arizona and how well the state treats innovation, equity, and long-term resilience. Arizona cannot afford to treat Long COVID research as someone else’s problem or someone else’s budget line. If we want a workforce that can show up, innovate, and lead, we need to build the infrastructure that keeps people from quietly dropping out of jobs, businesses, and community life. That means expanding beyond three brick-and-mortar study sites into more neighborhood clinics and mobile units that can reach Flagstaff, farm towns, and people who can’t tolerate summer heat or long drives. It means investing in innovative tools, remote monitoring, conversational AI, and richer data platforms that turn patient stories into decision-grade evidence instead of anecdotes. It also means using state-level funding and partnerships to stabilize research staffing, so Arizona stops losing trained coordinators and nurses to turnover just when their experience and earned trust among patients is most valuable. The disease burden of Long COVID is already reshaping our economy; the question for Arizona’s leaders, employers, and institutions is whether we will step up now, by backing more sites, more mobile outreach, and more tools, or pay the price later in lost productivity, shuttered small businesses, and preventable disability.
Sources:
- Shi J, Lu R, Tian Y, Wu F, Geng X, Zhai S, Jia X, Dang S, Wang W. Prevalence of and factors associated with long COVID among US adults: a nationwide survey. BMC Public Health. 2025 May 13;25(1):1758. doi: 10.1186/s12889-025-22987-8. PMID: 40361045; PMCID: PMC12070722
- Carazo S, Ouakki M, Nicolakakis N, Falcone EL, Skowronski DM, Durand MJ, Coutu MF, Décary S, Dialahy IZ, Drescher O, Canitrot E, McGinn CA, Latouche P, Laforce R, Dallaire C, Denis G, Piché A, De Serres G. Long COVID risk and severity after COVID-19 infections and reinfections: A retrospective cohort study among healthcare workers. Int J Infect Dis. 2025 Oct;159:108012. doi: 10.1016/j.ijid.2025.108012. Epub 2025 Aug 7. PMID: 40783164.
- Thaweethai, T., Donohue, S.E., Martin, J.N. et al. Long COVID trajectories in the prospectively followed RECOVER-Adult US cohort. Nat Commun 16, 9557 (2025). https://doi.org/10.1038/s41467-025-65239-4
- Graph Image Source https://crunchme.org/visual_images/%5B2026-02-22-01%5D.png
About The Author
Anisia Corona is a digital health entrepreneur and editor with 27 years of experience in healthcare. She is the founder of a digital health company. DxTx focused on strengthening the provider–patient relationship through AI-powered products for physicians, including a digital magazine that delivers proprietary and hard-to-find data and insights to clinicians. Anisia is the co-author of studies indexed by the National Institutes of Health and serves as a reviewer for NIH RECOVER research proposals and studies, as well as grant applications submitted to the United States Department of Defense. She also founded the Arizona Chapter of the AI Collective with a healthcare vertical, creating hands-on AI learning events that advance the use of AI in healthcare across Arizona.
Anisia Corona is a digital health entrepreneur and editor with 27 years of experience in healthcare. She is the founder of DxTx, a health tech company focused on strengthening the provider–patient relationship through AI-powered tools for physicians, such as clinical decision support for complex chronic conditions and conversational AI intake. Anisia also publishes a digital magazine that delivers proprietary and hard-to-find data and insights to clinicians. Anisia is the co-author of studies indexed by the National Institutes of Health and serves as a reviewer and on the Advisory Committee for NIH RECOVER research proposals and studies, as well as grant applications submitted to the United States Department of Defense. Anisia participates in working groups for the Coalition for Health AI (CHAI) as a Patient Advocate, approving best practices for the use of AI in healthcare. She also founded the Arizona Chapter of the AI Collective with a healthcare vertical, creating hands-on AI learning events that advance the use of AI in healthcare across Arizona.

Tanisha Prasad
Tanisha Prasad is an undergraduate student at The University of Queensland majoring in Molecular and Microbial Biotechnology, with a focus on clinical innovation and the commercialisation of biotech. Her background spans laboratory research and science communication, with experience shaped by programs ranging from the Australian Institute for Nuclear Science and Engineering to the San Francisco health-tech ecosystem through UQ Ventures. Currently an intern at DxTx and an assistant in the UQ Translational Biotech Startup Program, she works on early-stage health technologies and the systems needed to bring them into practice.




{kind=link}